Nutrition Department upgrades patient menus, room service ordering system
 |
CC food service worker Andre Russell delivers a tray including several items on the new menu (at left), including a tortilla-crusted tilapia with chipotle and lime, brown rice, steamed vegetable blend, spinach salad, and a seasonal fruit plate.
|
Clinical Center patients had 60 more food items to choose from when the Nutrition Department introduced its revised standard room service dining menu on June 28. The department added some new ingredients with international flare to appeal to patients from other cultures, as well as those who like ethnic cuisine, and augmented its selection of comfort foods for patients experiencing therapy side effects.
The new selections offer more vegetarian and whole grain items. The menus also upgrade the quality of several foods, including soups and cheeses; expand selections of herbal teas and baked potato toppings; and list flavors available for ice cream, popsicles, and gelatin. This is the second major redesign of the room service menu system since its initial launch in 2002. The project involved a great deal of behind-the-scenes work, such as tasting items,
 |
|
Cook Rene Brown prepares cheese quesadillas, one of the new ethnic menu offerings.
|
comparing ingredients and cost, coding each offering according to compliance with different diets, and training cooks and call center technicians.
David Folio, chief of the Nutrition Department, said ideas for the new menu were gathered from a variety of sources, including patient surveys, meal rounds by department staff, and feedback by the Patient Advisory Group and clinical dietitians. Incoming patients will find the new standard menu on tray tables in their rooms. The Housekeeping and Fabric Care Department places a menu when a room is cleaned after a patient is discharged.
The department redesigned its 30 specialized printed menus to make them physically larger with a larger type size and a more spacious layout.
According to Jennifer Widger, chief of the department’s food service section, the CC offers more than 160 different diets, and its computer system coordinates them and makes the room service program possible.
 |
|
Health technician Sherry Parker uses the new touch-screen technology on a computer in the department's call center, with the new patient menu for reference.
|
The department on May 17 also its computer system, which interfaces with CRIS, to display admissions, transfers, diet order changes, and discharges. The upgrade provides touch-screen technology on computers in the department’s call center so that health technicians can process patient room service orders more quickly. The Nutrition Department anticipates that the new technology will reduce time patients must spend placing their order.
Dietetic internship director retires
The department also said goodbye to Maureen Leser, director of the dietetic internship program for the past six years and clinical dietitian on 3NW, as she retired on August 1 after 21 years at the CC.
Under Leser’s guidance, four dietetic interns come to the CC every August for a 10-month supervised practice program in research dietetics to supplement academic coursework with clinical, food service, and administrative experience. They spend time with each of the department’s dietitians, and also perform off-site rotations. Competition for the internship is fierce: The CC receives 10
 |
|
Maureen Leser, retired dietetic internship director
|
applications for every space. The selection process resembles a residency matching program, with candidates and institutions ranking their choices. The American Dietetic Association requires an internship, and the CC is the top of many graduates’ list, so the CC receives many qualified candidates. So qualified, in fact, that the class that graduated on June 22 was the first to include two members with PhDs.
Madeline Michael, chief of clinical nutrition services, called Leser "the glue that holds the internship together" because she plays so many different roles for the interns: mentor, model, counselor, cheerleader, events planner, and friend. "We’re fortunate that Maureen has such a passion for her work," Michael said. "Her unit and her patients will miss her and the incredible things she accomplishes. Maureen really puts herself out there for the patients, empathizes with where they are in their treatment, and takes advantage of when they’re feeling well to learn more about them and what they need to nourish them during their stay."
Leser said she felt privileged to work at NIH, where the staff are so dedicated to research and patient care, and especially on 3NW, where she provided clinical nutrition services to patients enrolled in immunotherapy protocols or undergoing surgery. Registered dietitian Rachel Drabot assumed Leser’s clinical nutrition duties on 3NW; a search committee has formed to select the next dietetic internship program director.
Back to Top
Burst water pipe floods B1, B2 levels
 |
|
The water booster pump vibration eliminator that burst in the B1 chilled water supply area fit in the vertical space on the right side of the photo.
|
Late Tuesday evening, June 26, the Clinical Center experienced one of the worst floods in its history when a water booster pump vibration eliminator on a chilled water pipe burst and ran for 40 minutes before it was detected and stopped. The B1 and B2 levels of Building 10 experienced significant flooding, including Medical Arts, the NIH Library lower level, the CC’s Materials Management Department’s biomedical engineering and property management section, DCRI computer support services, and linen service. No one was injured in the incident or in the remediation period in the weeks following the flooding.
A vibration eliminator is a piece of rubber that joins two pipes transferring water and keeps it flowing. The pipe is fed by a pump sitting on the floor on a concrete slab to transfer water to coils in the air handling unit in the South entrance lobby.
NIH Library
The broken chilled water pipe was located in a utility room directly adjacent to the lower level of the NIH Library. Fortunately, recently installed compact shelves raised the level of the lowest tier of books and journals to six inches more than standard shelving. As a result, none of the four inches of standing water reached those items. Because of quick action to remove the soggy carpet and bring in dehumidifiers and fans, mold and mildew did not have time to develop. Staff from NLM’s preservation section came to the library shortly after the flood to salvage some expensive foreign language dictionaries and scientific treatises used by the library’s translations unit that were literally dripping wet.
The library reading room on the first floor remained open throughout. Aside from restricted access to the lower level and the print collections during the recovery process, the only major library service affected was document delivery, which fills about 500-600 requests each day for articles, primarily from the print journals on the B1 level. Because of damage and safety concerns, the first two days after the flood, no document requests could be downloaded, let alone filled. However, after the elevator resumed operation, the document delivery team regrouped and was able to obtain articles from other sources until scanners were back in operation and it was safe to again work in the area affected by the flood.
Medical Arts
 |
|
Wet ceiling tile debris fell on top of several computers and phones in workspaces on the B2 level.
|
Water did not accumulate as much in the library because it seeped through the floor of B1 seeped into the ceiling of B2 through the holes and cracks where utilities connect between floors, severely impacting NIH’s Division of Medical Arts and Printing Services. About 50% of the department’s equipment, including cameras, lenses, photography equipment, computers, and graphic design supplies, was destroyed and has to be replaced. About 35% of Medical Arts staff worked from home in the days following the flood, while others temporarily relocated to offices within Building 10. The TV operations center, which provides cable programming throughout the building, including to patient rooms, was turned off for about five hours on June 27 for water clean up, but sent its first transmission following the flood by 1 p.m. on June 28. The Center for Information Technology on July 2 rewired Medical Arts’ staff phones to the temporary support area on the 14th floor. The date for Medical Arts’ return to their B2 area is unknown at this time.
 |
|
Wet carpets soaked items on the floor, such as the bottoms of these cardboard storage boxes.
|
Biomedical engineering instrumentation and personal property management section (BEIP)
BEIP experienced a substantial loss of patient care-related equipment and supplies. A remediation crew and BEIP staff cleaned water from room B2S245, removed damaged boxes and supplies, removed and discarded soaked carpeting, installed dehumidifiers and fans, and opened up the walls to allow water to drain. The Housekeeping and Fabric Care Department (HFCD) sanitized the floors before the walls were repaired and painted, and the carpeting in the reception area replaced. Although the flood disrupted BEIP operations, all services critical to the CC were maintained through the activation of MMD’s emergency management plan and the partnership of all MMD Sections in stabilizing the area.
CC linen services
All linens stored in HFCD room B2S246 were sent out for laundering, and the area and adjoining corridors were cleaned by CC staff. Water was also removed from the scrubs storage area and the scrubs contained there were replaced. HFCD lost sheets, towels, slippers, and two computers with printers.
CC Facilities Management and DCRI computer support
The CC Department of Clinical Research Informatics’ B2L104 location housing several user support staff was practically destroyed. DCRI estimates that they have lost more than 50 computers, as the B2 office was a staging area for CC computer deployment, as well as storage for equipment provided to the nursing units. After about four days, all equipment from the area was removed and some salvaged. The entire area's furniture, carpeting, and ceiling will be replaced and the walls will be surveyed for water damage—a process that will take at least six weeks. The CC’s Office of Facility Management and the Duke room were also flooded on the B1 level, but staff were able to work in place once the water was cleaned up and dehumidifiers set up to dry out the area.
|
Timeline
|
- On Tuesday, June 26 at 9 p.m., Christian Ellenes, Facilities Operations Branch shift leader from 4 p.m. to midnight, received a call from the NIH power plant reporting a major drop in chilled water pressure throughout campus. His staff checked every chilled water system on campus and determined that a water booster pump vibration eliminator in Building 10 had blown out, causing major water damage to the carpet, ceiling tiles, computers, and other items on the B1 and B2 levels of Building 10. Access through the NIH Library was locked, so the NIH Police Department came to unlock the door.
- ORF emergency coordinator John Walker and CC Housekeeping and Fabric Care Department staff were notified. Elevators one through four, 13, and 14 were shut down until the water was contained. Staff secured the chilled water system at 9:45 p.m.
- The building automated system panel controlling heating and cooling equipment near the South entrance went down from the flood of water into it and required immediate repair. Additional personnel worked throughout the night and June 27 to remove water from all affected areas.
- Meanwhile, an electrician shut off power in the flooded areas for safety reasons. All electrical devices were unplugged and ground fault interrupters installed at each outlet to protect against electrocution.
- A sanitizing solution was applied to the floors and any wet drywall, rubber baseboard, and plywood was removed and replaced so that mold will not develop.
- NIH police implemented a security system from June 27 through July 9 to check badges of affected staff and clean up crews moving in and out of the area.
- On June 29 NIH staff received computer carts, plastic moving crates, face masks, and moving staff assistance to remove their equipment and supplies to their relocated office staging areas.
|
|
Status, contact information for each department affected
|
- Biomedical Engineering and Instrumentation Section: Contact information for staff has not changed.
- DCRI: Displaced staff may be contacted by their pagers and via email until the telephones are reconnected.
- Housekeeping and linen services: Contact information for staff has not changed.
- Library: The first floor reading room is open; access to the collections is limited to library staff only until the area is re-carpeted. Requests for journal articles and books can be made from the library’s Web site http://nihlibrary.nih.gov.
- Medical Arts: The department is in full operation from the 14th floor solarium, 14SD235. Photo services are operating from room 1N237, the old pharmacy by the main elevators. Please continue to submit your orders by e-mail, phone, or on-site. Visit http://medarts.nih.gov/docs/contact.htm or call 301-496-3221 for more information.
|
Back to Top
CC imaging study focuses on von Hippel-Lindau patients' hearing
by Shana Potash
 |
|
CC neuroradiologist and lead study author Dr. John Butman.
|
The results of an imaging study conducted at the Clinical Center could help doctors protect and preserve the hearing of people with the rare genetic disorder von Hippel-Lindau disease (VHL).
Researchers determined that bleeding from small, benign tumors near the inner ear can cause sudden hearing loss, and early intervention with surgery may be warranted rather than monitoring the slow-growing tumors over time. The study is published in the July 4 issue of the Journal of the American Medical Association.
Von Hippel-Lindau disease (VHL) causes the abnormal growth of benign and cancerous tumors in numerous parts of the body. This study focused on endolymphatic sac tumors (ELSTs). Ten years ago, researchers working in the CC first identified ELSTs and hearing loss as part of VHL disease, but the cause was not clear. Now a decade later, new research offers insight into the causes of hearing loss in VHL and treatment.
ELSTs and their connection to hearing loss are a curiosity because the endolympatic sac is on the temporal bone that contains the ear but is not part of the inner ear associated with hearing. Some cases of hearing loss in VHL can be attributed to large tumors on the sac that invade the hearing apparatus. But CC neuroradiologist and lead study author Dr. John Butman noticed, and set out to explain, why some patients lost hearing when they had only a very small tumor outside the sensory part of the ear.
 |
|
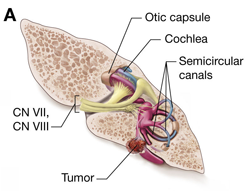
This illustration, courtesy of Alan Hoofring, shows the temporal bone in a VHL patient with a small ELST involving the endolymphatic sac. Bleeding from the tumor extends into the organs of balance and hearing.
|
He says he could see blood flowing from the endolymphatic sac into the inner ear in about half of the small tumors he imaged. Researchers then talked to patients to correlate the images with their symptoms. "It turned out virtually all patients who had evidence of bleeding had a sudden hearing loss," Butman explains. "For example, they were talking on the phone and suddenly their hearing went out, which is characteristic of a hemorrhage."
Other patients with small tumors experienced gradual hearing loss, but no bleeding. Butman says in those cases the ELST was disrupting the flow of fluids in the inner ear and causing and condition known as endolymphatic hydrops, which creates pressure, ringing in the ears, vertigo, and gradual hearing loss.
NINDS neurosurgeon Dr. Russell Lonser, senior author on the study, says the findings prompted a change in thinking about how to manage these tumors. Previous practice was a wait-and-see approach. Given that the tumors were benign, slow-growing, and their natural history was unknown, doctors monitored their growth and did not remove them until they became big enough to threaten hearing.
"It was believed these tumors probably would be best observed," Lonser says, "Now we believe they probably should be operated on very early on, as soon they are identified on imaging." Butman used CT imaging to study the bone and MR technology for the soft tissue and inner ear. He studied the inner ear with an imaging technique that is typically used for the brain to detect some of the cases of hemorrhage.
"Part of radiology is solving puzzles," Butman says. "Being able to figure out most of the story from imaging findings alone is very satisfying. Then having the clinical findings correlate so well with the imaging gives a sense of the solution to the puzzle. The fact that this has affected the thinking on how to manage patients is very nice."
Back to Top
Reception offers new fellows a chance to start finding their niche
 |
|
CC Director Dr. John I. Gallin welcomes two clinical fellows at the reception following orientation.
|
New clinical fellows met and mingled with Clinical Center and NIH leaders at the July 11 welcome reception. It's an annual tradition at the conclusion of the CC-sponsored orientation program that provides a unique setting for people from different countries, medical specialties, and experience to come together.
The fellows, who participate in a number of clinical training programs at NIH, including many accredited through the Accreditation Council for Graduate Medical Education, typically spend two to five years working in their own clinical specialties with senior clinical investigators.
The orientation and reception are just the beginning of a fellow’s time at NIH. The first year’s focus is clinical research and patient care at the Clinical Center. Subsequent training may involve clinical or basic research or a combination of both. Some of the training is offered at partner institutions such as National Naval Medical Center, Children’s National Medical Center, and Johns Hopkins University Hospital.
 |
|
Dr. Leighton Chan (left), chief of the CC Rehabilitation Medicine Department, talks with several fellows.
|
Dr. Robert Lembo, executive director for Graduate Medical Education in the Office of the Director’s Office of Intramural Training and Education, said that although graduate medical education at NIH is special in many ways, it "really boils down to this: an outstanding group of physician-scientists directing training programs in a unique, research intensive environment that provides cutting edge clinical care for a diverse population of patients with rare or complex disorders. This is an irresistible combination for talented, young physicians truly interested in advancing biomedical science and pursuing meaningful careers in academic medicine."
For some, the fellowship is a homecoming. NIAID fellow Dr. Christa Zerbe had worked at NIH since 1992 as an RN with NHLBI, then as a nurse practitioner with NIAID and NCI. She decided to go to medical school to understand more of the science behind her clinical work. Zerbe says that being both a physician and a nurse gives her a different perspective. "Nurses at the CC have so many great, unique opportunities to advance themselves educationally and professionally," she said.
Dr. Heidi Schambra, NIH Clinical Research Training Program class of 2001-2002, returned to NIH as a fellow in NINDS following four years of neurology residency at Brigham and Women’s Hospital and Massachusetts General Hospital (Partners). "I’m tremendously excited to be back. There are new projects, techniques, and people to work with. Things have grown so much since I was last here, in terms of what’s clinically and technologically available. That’s the great thing about the CC – the collaborative environment facilitates rapid, immediate, and intense research. It’s unlike any other place."
Several fellows mentioned the CC’s service ethic when sharing their first impressions after less than a week on campus. Dr. Jeanne Wang, one of the four fellows in the CC’s Department of Transfusion Medicine (DTM), said "the caliber of people concentrated on one campus is incredible. This place is special and you feel that the minute you start." Wang was particularly impressed with the friendliness and helpfulness of the CC hospitality staff. Dr. Jennifer Daniel-Johnson, another DTM fellow, remarked on the amazing learning opportunities and access to a large body of research expertise and worldwide medical resources, such as those provided by the NIH Library. "Everyone here goes the extra mile and goes out of their way to make every patient experience over the top. The service ethic is sincere," Wang said.
Zerbe, who like many of the clinical fellows, has not yet decided on a specialty, said, "NIH is vast, with so many opportunities, that you have to find an interest to cultivate and focus your career on. I want to find my niche."
Back to Top
'Nature Boy' pops up in Clinical Center courtyards
 |
|
"Wrapped Legs," by Keith Sharp. The toned silver gelatin print is part of the "Nature Boy" series at the CC.
|
No, you’re eyes aren’t deceiving you. There is an elf of sorts visiting the courtyards and walls of the Clinical Center, and he hopes to bring a smile to your face.
His name, or the name of the series of photographs to be more precise, is "Nature Boy," the work of Pennsylvania artist Keith Sharp. The exhibit includes 13 garden pieces from the "Nature Boy" series, which arrived in July, and eight framed wall pieces from other series by the artist that are coming to the Hatfield building’s west gallery in September.
The garden pieces came to the CC after gracing the greenery of the US Botanic Garden, which pressed the black-and-white photos between humidity-proof Plexiglas and placed them on stakes to create a whimsical juxtaposition of man and nature.
Lillian Fitzgerald, who works in the CC Office of Facilities Management as curator of the art exhibits, brought Sharp’s work to Building 10 as part of the CC's art program, which includes eight galleries with rotating exhibits and a permanent collection of approximately 2,000 original works of art.
The "Nature Boy" series combines Sharp’s interests in nature and self-portraiture by transforming himself into a tree creature, an image influenced by Greek and Roman mythology of people transforming into trees, the Druids, and Native American transformation stories. The framed wall pieces are photographs from other series that also contain humor and surrealistic elements.
Sharp said many people respond to the humor in his work, which he hopes will allow people to forget about their problems, if only for a little while, and bring joy to CC patients, visitors, and staff.
 |
"Running" by Keith Sharp
|
The element of surprise and mystery in Sharp’s visual puns is intentional. Although he documented the world in a straightforward way when he started in photography, Sharp soon began to tease the quirky elements out of his pictures and create staged, conceptual images. He now begins each series by sketching various ways that he can transform the everyday world through his imagination and make his viewers do a double-take.
The props and costumes Sharp assembled for his "Nature Boy" performances, of which a photograph is the end result, were created from natural and artificial materials, including bark, leaves, flowers, old clothes, fabric, plastics, paint, and glue.
"Juxtaposing elements within the photographs as well as between two photographs, I attempt to make the viewer look at ordinary life in new and unique ways. I am interested in pointing out the irony and contradictions in life—not everything is what it seems," he said.
Both portions of the exhibit leave the CC in November, so commune with "Nature Boy" while he’s here.
Back to Top
Ankylosing Spondylitis study seeks answers, shares knowledge
 |
|
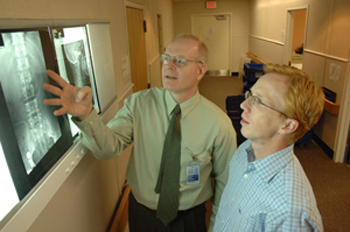
(from left) Dr. Michael Ward, a rheumatologist with NIAMS, shows CC patient Christian Drobnyk his X-rays and the places on his spine affected by Ankylosing Spondylitis.
|
by Jenny Haliski
When Christian Drobnyk was about ten years old, he began experiencing arthritic pain, mostly in his neck, but also in his pelvis. His mother began doing research into what might be wrong. Doctors found that Drobnyk carried a specific gene marker, HLA-B27, which is linked to a disease called Ankylosing Spondylitis (AS). The disease causes spinal joint inflammation, which over time causes the bones of the spine to fuse, resulting in difficulty performing daily activities. Although all the indications suggested that he might have AS, Drobnyk’s symptoms didn’t line up for an AS diagnosis for another 10 years. During this time, Drobnyk just wanted to figure out how to get back outside and play soccer.
Through a local support group for the Spondylitis Association of America, Drobnyk met Dr. Michael Ward, a rheumatologist with NIAMS and principal investigator for a study of the genetic determinants of the severity of AS. Drobnyk said he was happy to come to the NIH Clinical Center to participate in Ward’s study "to contribute to research so that the people who grow up after me figure out what’s going on more quickly and know how severe the condition is going to be."
Three-fourths of patients with AS are men, and the disease typically begins between the ages of 15 to 35. Inflammation and fusion often start in the sacroiliac joint of the pelvis and low back and later affect other parts of the spine. Bone fusion does not occur in everyone with spondylitis, but in severe cases, the spine fuses solidly, often resulting in a forward-stooped posture. AS patients must take care when exercising or driving, as their backs and necks are fragile.
AS is not a rare disease—one in every 1000 people have it—but it can take several years to diagnose because of the difficulty distinguishing mechanical back pain from the inflammatory arthritis of AS. AS is more prevalent than multiple sclerosis, cystic fibrosis, and Lou Gehrig’s Disease combined. AS patients may also develop other inflammatory conditions, such as heart valve disease, inflammatory bowel disease, and uveitis, an eye inflammation.
Treatments for its symptoms include physical therapy and exercise to preserve joint motion and flexibility, over-the-counter and prescription nonsteroidal anti-inflammatory medications (NSAIDs), and anti-TNF alpha drugs. There are currently no medications that are known to halt the fusion process, and patients progress at different rates so developing a customized treatment plan can be difficult. Ward hopes the study will provide physicians with genetic markers to predict whether a patient will have a slight or severe progression of the disease and assist in treatment recommendations.
Patients enrolled in the study come to the NIH Clinical Center every six months for examination of the joints, measurement of flexibility of the spine, and blood tests. X-rays are taken periodically. The study seeks to identify genes and genetic markers associated with AS and genes that influence the severity of AS. The HLA-B27 gene marker is present in 80 to 90 percent of individuals. It is believed that several other genes also increase a person’s risk of AS, but AS is not directly passed from parent to child.
Although Ward’s protocol does not provide treatment, Drobnyk said that building knowledge for himself and future patients through the study was a valuable experience for him. "The more you participate in the study of your own disease, the more you learn about it," noting that Dr. Ward answered his questions and monitored him during the study. "You give and you take back," Drobnyk said.
If you or someone you know has AS, contact the Patient Recruitment and Public Liaison Office at 1-800-411-1222 or TTY 1-866-411-1010 about study #03-AR-0131. The NIH-sponsored study is available to patients in locations other than Bethesda, Md. Participating institutions include Cedars-Sinai Medical Center in Los Angeles, the University of California-San Francisco, and the University of Texas at Houston.
Back to Top
A Clinical Center family
 |
|
Katie Parise, CC pharmacy technician, with her father, former NASA astronaut and CC patient Dr. Ronald Parise.
|
Katie Parise, pharmacy technician at the Clinical Center since January, may be a relatively new employee, but she already has a long history with Building 10.
Her mother, Cecelia, worked in the CC Pharmacy Department more than 20 years ago. The diagnosis of Parise’s father, former NASA astronaut Dr. Ronald Parise, with a stage IV glioblastoma in his temporal lobe brought the family back to the CC about a year and a half ago when conventional treatments had nothing left to offer.
After enrolling in several protocols, Dr. Parise met NCI’s Dr. Howard Fine, who is studying the use of avastin, a genetically engineered antibody that blocks the growth of new blood vessels in tumors, to slow or stop disease progression. Parise recalled that although other doctors said her father only had six months to live, once he received Dr. Fine’s experimental treatment, his tumor cleared up within two months. "It was a miracle, and it inspired me to get involved in the pharmacy here. This place is amazing with everything that they do for people," she said.
Parise hopes to attend pharmacy school in the fall of 2008. In the meantime, she says the experience of processing physician orders in the pharmacy’s unit dose area is a "great way to learn the business." Working at the CC also keeps her close by to accompany her father to his NCI protocol appointments twice a month and his weekly speech therapy in the CC Rehabilitation Medicine Department.
Dr. Parise said he’s proud that both his wife and daughter have contributed to clinical research, adding that his wife saved his life by drawing on her health care experiences at the CC to research his condition and contact doctors.
The CC staff he’s met have also been very helpful, he said. "It’s a terrible mess getting a tumor that’s potentially fatal, but guys like Dr. Fine did a tremendous job. And here we are. We’re living again."
Back to Top
Summer brown bag series shares leadership coaching tips
 |
|
Executive and leadership development coach Cynthia Way leads the group through an interactive exercise in the seminar on avoiding overwork.
|
The Clinical Center’s Office of Workforce Planning and Development in July hosted the last of its summer brown bag sessions on leadership development. The five monthly presentations starting in March provided staff with an opportunity to hear about and discuss workplace development topics with executive and leadership development coaches.
Dr. Deb Gardner, chief of workforce planning and development, said the series grew from the success of CC managers’ development courses and their requests for additional exposure to management topics. Gardner said the summer series also proved really popular, with about 40 to 50 CC staff attending each session.
The following are some of the concepts and tips presented in the summer sessions for staff who were unable to attend. Gardner’s team welcomes staff to participate in the fall monthly brown bag sessions, which will start in September and will explore more topics around effective performance management.
"Communicating for Outcomes"
Frank Ball shared a five-step feedback communication model based on the Gilburg Leadership method. The five steps are data collection, feeling, judgments, wants, and willingness. The first step reports behavioral data on what occurred and was observed -- imagine what a video camera could capture if one were on nearby, without judgment or interpretation. Feelings could be one of four fundamental categories: glad, sad, mad, or afraid. Judgments involve interpretations, conclusions, or beliefs about the other person or situation. The fourth step involves expressing what you want from the other person, in positive terms of the relationship and future behavior. Finally, consider and share with your colleague what commitment you are willing to make to help the other person reach that goal.
"Five Dysfunctions of a Team and How to Avoid Them"
Dr. Arleen LaBella asked CC staff to reflect on the characteristics of an effective team, which is defined as a small number of people with complementary skills who are committed to a common purpose, shared goals, and mutual accountability for the work. She shared five common pitfalls addressed in Patrick Lencioni’s book "The Five Dysfunctions of a Team": absence of trust, fear of conflict, lack of commitment, avoidance of accountability, and inattention to results. To help a team improve performance, LaBella recommended selecting any incident and then reflecting on three questions: What did we observe? What have we learned? What can we do differently?
"Avoiding Karoshi"
With her simultaneously interactive and Zen presentation, Cynthia Way reminded the group that what you focus on, you get more of, and what you seek is what you find. Constant stress and overwork begets more stress and overwork. "Karoshi," the Japanese word for "death by overwork," describes not only tension but also the stress-related illnesses associated with overworking. Way encouraged the group to find one positive thing they could do that would make a big difference in their stress levels, such as taking a walk at lunch with co-workers.
"Difficult Conversations"
Paula Lowe highlighted the personal and organizational costs of avoiding difficult conversations -- where the stakes are high, opinions vary, and emotions are strong -- and shared techniques for constructively addressing them. According to Lowe, what is important in a tough situation is frequently not expressed, and often is at some level anxiety around a threat to a basic human need, such as competence. When we perceive that our needs are at risk, we have a physiological reaction, based on the fight or flight instinct. To manage emotions and engage our logic, avoid "charged" language or judgments that might create defensiveness unnecessarily. Keep your voice at a normal conversational level and observe and act on the other person’s non-verbal cues. Paraphrase what the other person said to show that you’re listening and give them a chance to correct misunderstandings. It’s easier to be honest and open if you start from a place of respect and good intentions.
"Using the Myers-Briggs to improve team performance"
Dr. Hany Malik shared how appreciating and leveraging the personality preferences described by the Myers-Briggs Type Indicator, the most commonly used psychological profile system in the U.S., in a team setting can add richness and improve the quality of work products. The 16 personality types are about preferences, not about knowledge, skills, or abilities; there are no right or wrong preferences. Identifying your team members’ MBTIs can help with understanding why individuals act as they do and facilitate team discussions around what members need to be successful.
Back to Top
Summer students arrive at the Clinical Center
Undergraduate, graduate, and medical students come to NIH each summer to complete internships with institutes and centers and gain a unique perspective on clinical research.
 |
|
(from left): Charles Hatt; Amritha Nayak; Dr. Scott Paul, a senior clinician within the CC's Rehabilitation Medicine Department's Physical Medicine Section; Frances Chien; and Patricia Turnquist.
|
Chien, Nayak, and Hatt’s project is studying new equipment to apply stereophotogrammetry, a form of 3D surface imagery, on the whole body.
Turnquist’s project is studying the reliability and validity of the Quality Muscle Assessment, which objectively measures force production in patients with neuromuscular disease.
Turnquist, a recent physical therapy graduate of University of Southern California, joined a team working with normal volunteers to understand how investigators can apply the tool to test muscle groups that are affected by disease processes.
"It’s a great opportunity to come here and work with top researchers in physical therapy, and medicine in general," Turnquist said.
Borman and Weeks are working with Dr. Jay Lozier in the Department of Laboratory Medicine’s
 |
|
(from left, back row): Zachary Borman, James Stoner, and Brian Weeks. (front row): Maria Belarezo, Ina Sen, and Kelly Moltzen.
|
Hematology Service to analyze the DNA sequence of the canine X chromosome for applications to human disease. Belarezo, Stoner, and Sen’s mentors are Jim DeLeo and Carl Leonard in DCRI, which is developing a biomedical knowledge discovery system for all principal investigators to dig deeper into clinical data. Moltzen is a summer student with the Nutrition Department working in the Metabolic Clinical Research Unit with body composition data.
Back to Top
CC HIV/AIDS counselor retires after 20 years
 |
|
Tina Levin, former CC HIV counseling coordinator, retired on June 29.
|
Tina Levin, social worker and HIV counseling coordinator in the Clinical Center’s Social Work Department, has assisted hundreds of people in crisis as they process living with HIV/AIDS. Some were recently diagnosed, while others wrestled with on-going issues related to life with a stigmatized disease. According to Levin, the Chinese character for crisis also means opportunity, a concept she applied to her work. "If someone in crisis lets you in and allows you to work with them, it’s a privilege," Levin said.
Levin found her passion for social work when she was almost 40 years old. When she returned to school to become a social worker, her fieldwork placed her in Washington Hospital Center’s burn unit. She responded to a sign there seeking social work students at NIH and spent two summers at the CC working with patients with endocrine disorders, lupus, arthritis, and musculoskeletal disease. After graduation, she began full-time work with cancer and HIV patients.
Joining the CC as a new social worker in the late 1980s when HIV/AIDS was still relatively new, Levin said she found "incredible opportunities for professional growth." From giving presentations to leading support groups, Levin developed expertise in the field while satisfying her love of working with people. "You think you’re going in to help them, but you come out enriched yourself," she said.
Department Chief Dr. Adrienne Farrar said Levin is "an outstanding clinician, teacher, and an expert in the psychosocial consequences of HIV/AIDS infection. She has given her all to these endeavors. Tina has also been a wise and empathetic manager in the SWD who is greatly respected by staff and will be truly missed by members of the department’s management team. She has tremendously contributed to all of us by not only teaching us how to be professionals, but also how to be well-rounded human beings." CCMD Chief Dr. Henry Masur said that Levin was "available, informed, and proactive" during her career, and "had the vision and courage to work in areas that others did not want to wade into."
According to Levin, Jewish tradition says that if you save a life, you save the world. "I really believe that. I went to work here at the Clinical Center knowing that if I died the next day, there’s nothing I would have done differently."
After retiring on June 29 after 20 years of service, Levin will spend a few months pondering her next move, which might include private practice or teaching in local social work schools. Courtney Duncan and Jeasmine Aizvera in the SWD will absorb Levin’s responsibilities.
Back to Top
Mandatory emergency generator tests scheduled for third Saturday each month
The third Saturday of every month, starting August 18, the NIH Office of Research Facilities, in collaboration with the Clinical Center Facilities Management, will conduct mandatory monthly emergency generator tests to comply with the Joint Commission's hospital accreditation standards.
Emergency power testing will occur in the Hatfield building between 8-11 a.m. There will be a total outage, both emergency power and normal power. The emergency power will come back on by generator in 10 seconds. At that time, the emergency power will come on only for the emergency lighting and receptacles. It is planned that normal power will be back on in approximately 30 minutes. Upon return to normal power, there will be three to five seconds where this is a loss of emergency power and then all systems will return to normal.
Testing will occur in the Magnuson building and ACRF from 1-4 p.m. During this time period, emergency power only will be affected. Normal power will not be affected. Building occupants will notice a 10-second outage in emergency power during this testing period.
Back to Top
CC alters staff TB test requirement
In the past, all Clinical Center employees who provided patient care were required to have annual skin test surveillance for tuberculosis. In 2005, CDC issued updated guidelines for preventing tuberculosis in health-care settings. Based upon the criteria for institutional assessment in the revised guidelines, the CC is categorized as a low-risk setting for occupational exposure to Mycobacterium tuberculosis.
Consistent with these guidelines, the Occupational Medical Service will modify its tuberculosis-screening program. OMS will continue to perform initial two-step tuberculin skin testing (TST) for newly hired CC employees. Only health care workers in high-risk occupations will be recalled for annual TST. All other employees can have annual skin testing by OMS by appointment, but the annual skin test will no longer be a mandatory requirement. Annual recall letters will only be sent to those employees required to have annual TST.
Walk-in TST clinic in OMS ended July 31. Employees requesting voluntary TST should call 301-496-4411 to schedule their appointments. CDC’s guidelines are available online at www.cdc.gov/mmwr/preview/mmwrhtml/rr5417a1.html.
Back to Top
Introduction to clinical research course accepting registrations
Registration for the 2007-2008 "Introduction to the Principles and Practice of Clinical Research" course starts August 1. The course will run from October 15, 2007, through February 25, 2008. Classes will be held on Monday and Tuesday evenings from 5 p.m. to 6:30 p.m.
There is no charge for the course; however, the textbook, Principles and Practice of Clinical Research, Second Edition is suggested for the course. A certificate will be awarded upon successful completion of the course, which is based on a final examination.
Course Objectives include developing familiarity with the basic epidemiologic methods involved in clinical research; the ability to discuss the principles involved in the ethics of clinical research; the legal issues in clinical research; the regulations involved in human subjects research, including the role of IRBs in clinical research; familiarity with the principles and issues involved in monitoring patient-oriented research; and the ability to discuss the infrastructure required in performing clinical research and an understanding of the steps involved in developing and funding research studies.
This course will be of interest to physicians and all other health professionals planning for a career in clinical research. A course in biostatistics, such as STAT 200 or STAT 500, currently offered at the Foundation for Advanced Education in the Sciences may provide supplemental benefit to those enrolled in the class.
For additional information or to register, please visit the course website at http://www.cc.nih.gov/training/training/ippcr.html or call the Office of Clinical Research Training and Medical Education at 301-496-9425.
Back to Top
News Briefs
New process addresses protocol attribution
CRIS, the Clinical Research Information System, will soon implement a new process that will make it easier to track medical orders and services according to a patient's protocol. SEe it in action at the CRIS Information Booth on August 7. STaff will be outside the second floor cafeteria from 8-9:30 a.m. and 11 a.m.-1 p.m.
to answer your questions. The Department of Clinical Research Informatics coordinated with the Medical Executive Committee to develop the new protocol attribution process. More information and training are available online,
http://cris.cc.nih.gov
. CRIS staff also are available to answer your questions about this new process. Call 301-496-8400.
Registration deadline for Principles of Clinical Pharmacology course
August 23 is the deadline to register for the 2007-2008 CC Principles of Clinical Pharmacology course, which will be held Thursdays from 6:30 p.m. to 7:45 p.m. in Lipsett Amphitheater and will run through April 24, 2008. Course information, including online registration, is available at http://www.cc.nih.gov/training/training/principles.html or by calling 301-435-6618.
Spotlight features CC’s clinical research awareness Web site
The June 25 NIH Health Information Spotlight, a weekly health information Web page update, featured the CC’s new Web site discussing the benefits of clinical research and how to participate. Explore http://clinicalresearch.nih.gov today—because lives depend on it.
Back to Top
New clinical research protocols
The following new clinical research protocols were approved in June:
A Phase I Study of BMS-354825 (DASATINIB) in Children with Recurrent/Refractory Solid Tumors or Imatinib Resistent PH Plus Leukemia, 07-C-0166, Elizabeth Fox, MD, NCI
Phase II Study of Metastatic Melanoma Using Lymphodepleting Conditioning Followed by Infusion of Anti-gp100:154-162 TCR-Gene Engineered Lymphocytes, 07-C-0174, Steven A. Rosenberg, MD, NCI
Phase II Study of Metastatic Melanoma Using Lymphodepleting Conditioning Followed by Infusion of Anti-MART-1 F5 TCR-Gene Engineered Lymphocytes, 07-C-0175, Steven A. Rosenberg, MD, NCI
A Phase II Study Using Sort-Term Cultured Anti-Tumor Autologous Lymphocytes Following a Non-Myeloablative Lymphocyte Depleting Chemotherapy Regimen in Metastatic Melanoma, 07-C-0176, Steven A. Rosenberg, MD, NCI
Noninvasive Optical Imaging of the Effects of External Spectral Filters on Macular Autofluorescence in Pseudophakic Eyes, 07-CH-0169, Robert F. Bonner, PhD, NICHD
The Effect of Diet on Vascular Disease: A Study of Pre-Menopausal African Amercian and Caucasian Women, 07-DK-0163, Anne E. Sumner, MD, NIDDK
Efficacy of WT1 and PRI Peptide Vaccination for Patients with Low Risk Myeloid Malignancies, 07-H-0159, Katayoun Rezvani, MD, NHLBI
Treatment of Pulmonary Hypertension and Sickle Cell Disease with Sildenafil Therapy, 07-H-0177, Roberto F. Machado, MD, NHLBI
Disclosure of a Cystic Fibrosis Diagnosis to a Dating Partner, 07-HG-N162, Kimberly Kaphingst, ScD, NHGRI
An Open Label Non-Randomized Dose Escalating Trial to Assess Safety and Tolerability of Alb-Interferon Alfa 2b Every Two Weeks with Ribavirin Among HIV/HCV Coinfected Individuals, 07-I-0001, Shyamasundaran Kottilil, MD, NIAID
Treatment for Growth Failure in Patients With X-Linked Severe Combined Immunodeficiency (XSCID): A Phase 2 Study Assessing Safety and Clinical Response to Treatment with Insulin-like Growth Factor-1 (IGF-1), 07-I-0171, Suk S. De Ravin, MD, NIAID
A Phase I Open-Label Study of the Safety and Immunogenicity of a Recombinant DNA Plasmid Vaccine, VRC-AVIDNA036-00-VP, Encoding for the Influenza Virus H5 Hemagglutinin Protein Administered Intradermally in Healthy Adults, 07-I-0172, Julie E. Martin, DO, NIAID
Suppression and Facilitation of the Motor Cortex by Stimulation of the Cerebellum in Patients with Dystonia and Healthy Controls, 07-N-0165, Mark Hallett, MD, NINDS
Back to Top
Research volunteers needed for studies
To participate in any of the following studies, call 1-866-444-2214 or TTY: 1-866-411-1010.
Muscular leg painVolunteers with muscular leg pain caused by blocked arteries that occurs with activity but improves with rest may be eligible for this new study (04-H-0143).
HIV-positive volunteersHIV-positive individuals who are no longer taking anti-HIV medications with CD4+ counts of 300 or greater are needed for a research study (05-I-0123). Compensation provided.
Neurofibromatosis type 1An NIH study seeks adults with neurofibromatosis type 1 for a protocol (06-HG-0134). All study-related tests are provided at no cost.
Back to Top
Upcoming Events
Clinical Center Grand Rounds for Clinical Fellows
August 1, 2007
Separating Wheat from Chaff: Critical Reading of the Biomedical Literature
Michael M. Gottesman, M.D.
Deputy Director for Intramural Research, Office of the Director, NIH
August 8, 2007
Educating for Professionalism: Pitfalls and Opportunities
Deborah E. Powell, M.D.
Dean and Assistant Vice President for Clinical Sciences, University of Minnesota Medical School
August 15, 2007
Ethics, Race, and Cancer Mortality in the United States
Victor R. Grann, M.D., M.P.H.
Clinical Professor of Medicine, Epidemiology, and Health Policy and Management, College of Physicians and Surgeons and Mailman School of Public Health, Columbia University
August 22, 2007
Simulation in Health Care
Amy Guillet Agrawal, M.D.
Director, Clinical Simulation Service, Critical Care Medicine Department, NIH Clinical Center
August 29, 2007
Shifting the "On-Call" Paradigm: Translating Sleep and Safety Science into Practice
Christopher P. Landrigan, M.D., M.P.H.
Director, Sleep and Patient Safety Program, Brigham and Women’s Hospital;
Research Director, Children’s Hospital Boston; Assistant Professor of Pediatrics and Medicine, Harvard Medical School
Back to Top
Clinical Center News, National
Institutes of Health, Building 10, 10 Center Drive, Room 12C440, Bethesda, MD 20892-1504. Tel: 301-496-6787.
Fax: 301-402-2984. Published monthly for CC employees
by the Office of Communications, Patient Recruitment, and Public Liaison. News, article ideas,
calendar events, letters, and photographs are welcome.
Back to Top
|
|

 The information on this page is archived and provided for reference purposes only.
The information on this page is archived and provided for reference purposes only.